Corneal cross-linking is a treatment designed to strengthen the cornea when it is becoming weaker and more unstable, most commonly in keratoconus and other corneal ectasias. It works by combining riboflavin (vitamin B2) and UV-A light to create new chemical bonds within the cornea, helping it resist further shape changes.

To strengthen the cornea and help stop progressive ectasia from getting worse.
Patients with progressive keratoconus, post-LASIK or post-PRK ectasia, and some other corneal ectasias.
Usually an outpatient procedure.
Вepends on the protocol. Epi-on is faster to recover from, while epi-off involves longer epithelial healing.
Corneal cross-linking is designed to solve a very specific problem: a cornea that is becoming biomechanically weaker and progressively changing shape. In keratoconus and corneal ectasia, the cornea can thin and bulge forward over time, leading to worsening distortion and reduced visual quality. Cross-linking helps make the cornea stiffer and more resistant to further deformation.
This is important because many patients assume every treatment is meant to “fix vision.” Cross-linking is different. Its main purpose is to preserve the eye’s future by slowing or stopping progression. Vision may improve in some patients, but the primary goal is stabilization.
When
Timing matters. Cross-linking is generally most valuable when progression is identified early enough to preserve corneal structure before more advanced distortion develops. Mayo Clinic notes that cross-linking may reduce the risk of progressive vision loss by stabilizing the cornea early in the disease.
In practice, this means the treatment is usually not offered simply because someone has keratoconus. It is offered because the cornea appears to be getting worse. In children and younger patients, this decision may be made earlier because progression can be more aggressive. ELZA’s current page also notes that the most powerful epi-off approaches are still reserved for situations where maximum biomechanical effect is needed, such as particularly aggressive disease in children.

How
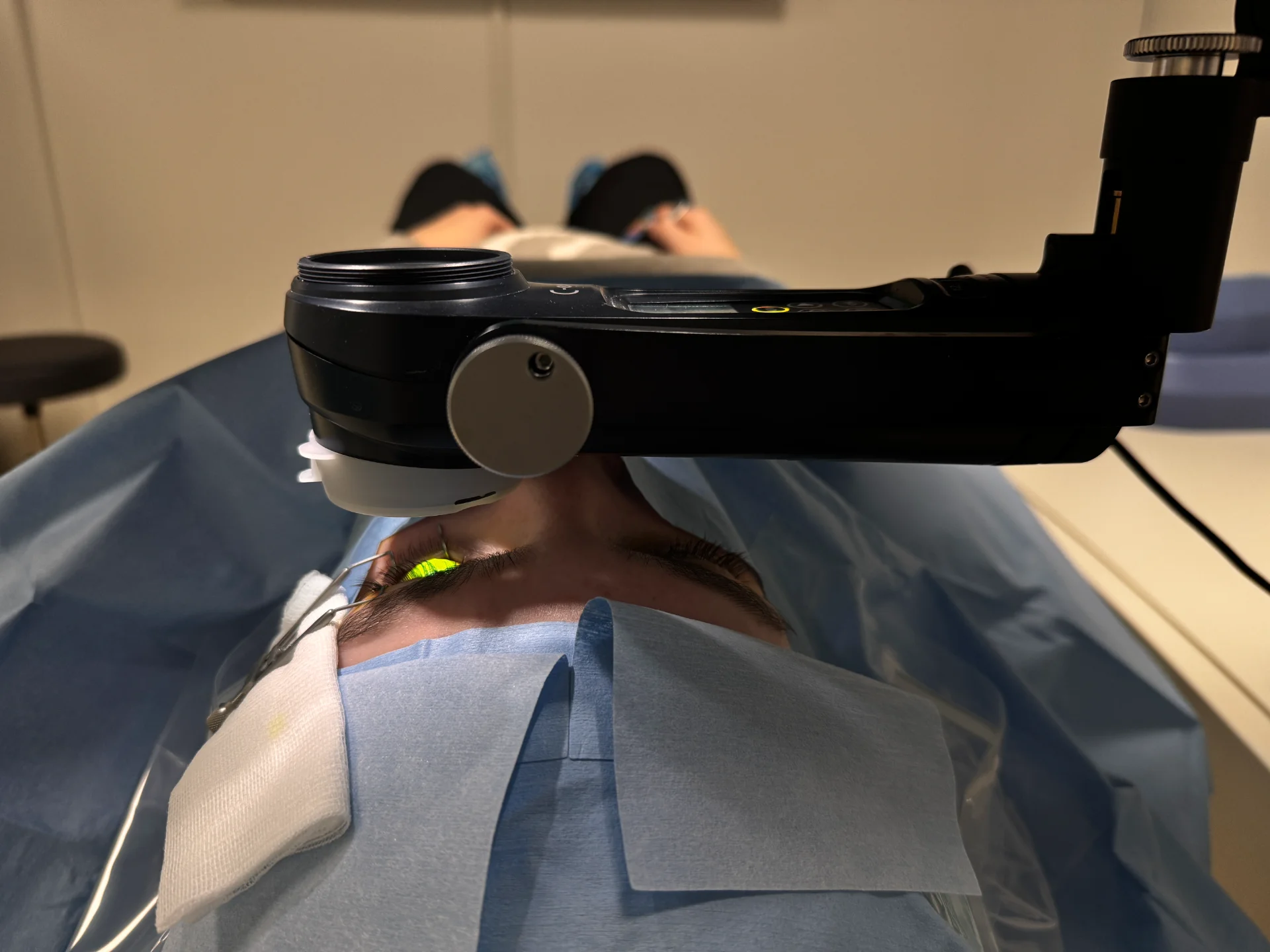
Cross-linking combines riboflavin eye drops with UV-A light. Together, they trigger a photochemical reaction inside the corneal stroma, the main structural layer of the cornea. This reaction creates new cross-links between collagen molecules, binding them more tightly together and making the cornea mechanically stronger. ELZA’s current page states that this stiffening effect is immediate and that the cornea becomes substantially stiffer after treatment.
ELZA’s page also explains that cross-linking has effects beyond mechanical stiffening. UV-A activated riboflavin can generate reactive oxygen species with antimicrobial effects, and the cross-linking process can increase resistance to enzymatic digestion and may reduce corneal swelling. These added effects are part of why cross-linking technology is also relevant in fields such as infectious keratitis treatment.
São utilizadas gotas oculares para adormecer o olho, pelo que o tratamento é geralmente confortável.
O doente fica sentado, deitado ou numa lâmpada de fenda, consoante a técnica utilizada.
O processo completo demora cerca de 45 minutos a uma hora, mais uma vez dependendo da técnica utilizada.
Is it Safe?
CXL’s safety has been demonstrated time and time again in many studies. Currently (as of May 2025), more than 3,000 peer-reviewed scientific articles can be found in the medical database, and our group has contributed over 160 of them.
A major safety principle in traditional CXL is protecting the corneal endothelium by ensuring enough riboflavin-soaked tissue remains between the UV treatment zone and the deepest cell layer.
The main limitation is that cross-linking is primarily a stabilization treatment. It does not guarantee better unaided vision, and it does not eliminate the need for other treatments such as specialty contact lenses or, in more advanced cases, additional corneal procedures. Also, not every protocol is equally effective in every clinical situation.
O último efeito secundário benéfico do fortalecimento da córnea que o CXL consegue é o facto de poder reduzir o edema da córnea, ajudando a córnea a manter a sua forma e clareza e, em última análise, a acuidade visual dos doentes.

Treatment
Over the years CXL for keratoconus and other corneal ectasias has evolved, and today various protocols exist. The treating ophthalmologist needs to assess which technique is scientifically sound enough to be used on a case-by-case basis.
Eis as abordagens de tratamento do CXL para aectasia atualmente disponíveis:
Porquê nós?
At ELZA, cross-linking is not just one treatment among many. It is one of our defining areas of expertise. Our current CXL page states that Prof. Farhad Hafezi was part of the Zurich team that developed the first UV irradiation lamp used for clinical cross-linking, and the page emphasizes ELZA’s long-standing role in the scientific development of the field.
We also do not treat cross-linking as a one-size-fits-all procedure. ELZA’s own pages explain that the treating ophthalmologist must understand the full range of scientifically sound protocols and decide which approach is appropriate on a case-by-case basis. That includes epi-off, accelerated approaches, and evolving epi-on methods, as well as customized treatment pathways such as ELZA-PACE. Our institute also highlights dedicated support for international patients and online consultations, making specialist access easier for patients traveling from abroad.
CXL treatment benefits from strong experience with the corneal surface, not only basic excision.
ELZA highlights published expertise and international reputation in cornea and ophthalmology.
ELZA offers dedicated pathways for international patients and online video consultations.
FAQs
Its main job is to stop progression. Some patients may notice some improvement, but that is not the main guarantee.
Discomfort depends on the protocol. Epi-off is usually more uncomfortable during healing than epi-on.
That depends on the protocol. The traditional Dresden protocol uses 30 minutes of UV-A at 3 mW/cm², while accelerated versions shorten the treatment time using higher intensity.
Often yes. Cross-linking stabilizes the cornea but does not necessarily eliminate the need for visual correction.
In epi-off, the surface epithelium is removed before treatment. In epi-on, it is left in place and special strategies are used to help riboflavin penetrate. Epi-on is generally more comfortable, while epi-off still remains important for cases needing the strongest biomechanical effect.
O CXL foi desenvolvido nos anos 90 como um tratamento inovador para fortalecer a córnea e travar condições de afinamento progressivo como o ceratocone.
A investigação inicial foi liderada pelo Professor Theo Seiler em Dresden, Alemanha. Ele e a sua equipa investigaram métodos para reforçar córneas enfraquecidas através da indução de ligações moleculares adicionais - chamadas ligações cruzadas - entre fibras de colagénio utilizando luz ultravioleta (UV) combinada com a vitamina riboflavina.
Em 1999, o Professor Seiler mudou-se para Zurique, na Suíça, onde se juntou ao (na altura) Dr. Farhad Hafezi. Juntos, realizaram alguns dos primeiros estudos clínicos sobre CXL no Instituto ELZA e em centros afiliados, desenvolvendo os protocolos que formaram a base do tratamento moderno com CXL. Zurique tornou-se um centro internacional de inovação clínica em cross-linking corneano.
Durante estes anos de formação, o tratamento era conhecido por vários termos, incluindo o cross-linking do colagénio da córnea (CCL) e o X-Linking. Em 2006, num congresso internacional realizado em Zurique, os especialistas chegaram a um consenso sobre o termo "cross-linking corneano" (CXL), que desde então se tornou o padrão global.
Graças ao seu trabalho inicial e às inovações contínuas da equipa do Instituto ELZA, o CXL está hoje estabelecido em todo o mundo como o tratamento de referência para travar a progressão do ceratocone e melhorar os resultados dos doentes.
Entrar em contacto
Durante o horário de expediente.
Envie-nos um e-mail.
Marque uma consulta e venha ver-nos.
Obrigado por escrever uma avaliação no Google.
Contacte-nos aqui e entraremos em contacto consigo.
Consulta online com zoom para os nossos pacientes internacionais.
Contacte-nos aqui e entraremos em contacto consigo.
Contacte-nos aqui e entraremos em contacto consigo.
Mantenha-se informado & receba o boletim informativo
Aderiu com sucesso à nossa lista de subscritores.
Receber e informar sobre o boletim informativo
Eles estão a ser bem sucedidos na nossa lista de contactos.
Por favor, melhore a sua assinatura, ao clicar no link do e-mail, que nós já enviámos.