If you (or your child) have recently been diagnosed with keratoconus – or suspect something is not right with your vision – this page will help you understand what the condition is, what symptoms to watch for, how it is diagnosed, and what treatment paths may be available.

What is Keratoconus, and why it affects vision.
Common symptoms and how they often begin.
Possible causes, risks, factors, behaviours.
How doctors confirm the diagnosis.
What treatment options are available?
What results can you expect after treatment.
Overview
Keratoconus is a condition in which the cornea – the clear front surface of the eye – becomes thinner and gradually bulges forward into a more cone-like shape. Because the cornea helps focus light, these changes can cause vision to become blurred, distorted, and harder to correct.
Keratoconus often develops gradually. Many people first notice that their glasses no longer seem to work well, that vision becomes increasingly irregular, or that driving at night feels more difficult than before.
The good news is that modern corneal diagnostics and treatment options can help doctors assess the condition more precisely and guide patients toward the next appropriate step.
Symptoms
Symptoms often appear gradually. At first, keratoconus may look like ordinary worsening eyesight, which is one reason the condition can go undiagnosed for some time.
If you are experiencing any of the following symptoms you should book an appointment with a cornea specialist, especially if one or more risk factors apply to you. The faster your symptoms deteriorate, the faster you should book an appointment. If you have already been diagnosed with keratoconus, please look out for symptoms in your family, especially in your children or nieces and nephews, and let them have screened by a specialist.
Vision may seem distorted, hazy, shadowed, stretched, or less sharp even with glasses.
You may notice increased glare, halos around lights.
The astigmatism in your glasses increased over the last 2 years.
You do not like driving at night, especially when it rains.
Your optician cannot correct your vision with glasses and glasses do not really help.
You frequently rub your eyes, either because you have an allergy or because eye rubbing has become a habit.
One eye may become noticeably worse than the other, making reading or daily tasks more frustrating.
Causes
There is not always one single cause. Keratoconus is generally thought to be linked to a combination of genetic predisposition and environmental or mechanical factors.
Some patients have a family history of keratoconus. Frequent eye rubbing is also commonly discussed as a risk factor, especially in people with allergies or long-term eye irritation.
Family history may increase the likelihood of developing keratoconus.
Frequent rubbing may be associated with progression and is commonly discouraged.
Itching and chronic irritation can make eye rubbing more likely.
Early assessment helps doctors understand whether the condition is stable or changing.
Diagnosis
Diagnosis usually involves a full eye examination together with detailed corneal imaging. The aim is not only to identify keratoconus, but also to understand how advanced it is and whether it appears to be progressing.
To diagnose keratoconus, we start by reviewing your vision history. After that, we’ll perform a series of specialized eye exams to get a clear picture of your cornea.
Your specialist will review symptoms, prescription changes, and how your vision has been changing over time.
Topography or tomography helps doctors measure the shape of the cornea in much greater detail.
Measuring thickness helps show whether the cornea is becoming thinner in a pattern consistent with keratoconus.
A good diagnosis gives patients more than a print-out. It helps define severity, assess progression, and choose appropriate treatment.

We have a close look at your cornea through the biomicroscope and evaluate your prescription and whether your astigmatism has changed over time.

An essential exam that can detect even early stages of the disease. A detailed map of the cornea’s, its epithelium and thickness is created. We use the most modern variant, combining optical coherence tomography (OCT) and placido-based measurements (MS-39).

We use a sophisticated Scheimpflug imaging system that takes more than 4.000 images per second to analyze how your cornea reacts biomechanically (CosVis ST).

As global leaders in keratoconus treatment, ELZA’s surgeons have developed a number of new techniques to not only stabilize keratoconus, but to improve the patient’s vision and visual quality.
ELZA’s medical director Prof. Farhad Hafezi officially is the most productive scientist on the topic globally, followed by ELZA’s Dr. Emilio Torres and Dr. Mark Hillen at numbers 2 and 5.

Keratoconus is a disease of young people and most common and most aggressive in children (8 to 15 years) and adolescents (10 to 19 years).
Our group has one of the longest international experiences in the treatment of keratoconus in children and adolescents. We were the group that published the first large study on CXL in children and were the first to recommend immediate CXL in young patients under 20 years, once the disease has been diagnosed.
Treatment paths
Regardless of the degree of keratoconus, there are several treatment options, and some of them (ELZA epi-on CXL, ELZA-sub400, ELZA-PACE) have been pioneered by us, and used today throughout the world. These options can be divided into two approaches: stopping keratoconus progression and improving your vision.
Corneal cross-linking (CXL) is a treatment designed to strengthen the cornea and halt the progression of keratoconus, which is crucial for preventing the disease from worsening. If the cornea becomes too thin, it can rupture, leading to a central scar and potential legal blindness. This was a common outcome for many patients before CXL became available in clinical ophthalmology in Zurich, Switzerland, in the early 2000s, with Farhad Hafezi as part of the pioneering team. Since CXL was introduced, the need for corneal transplants has dropped by up to 50% – early detection allows for early CXL treatment, stopping the disease from progressing and preserving useful vision.
Read about Corneal cross-linking (CXL)

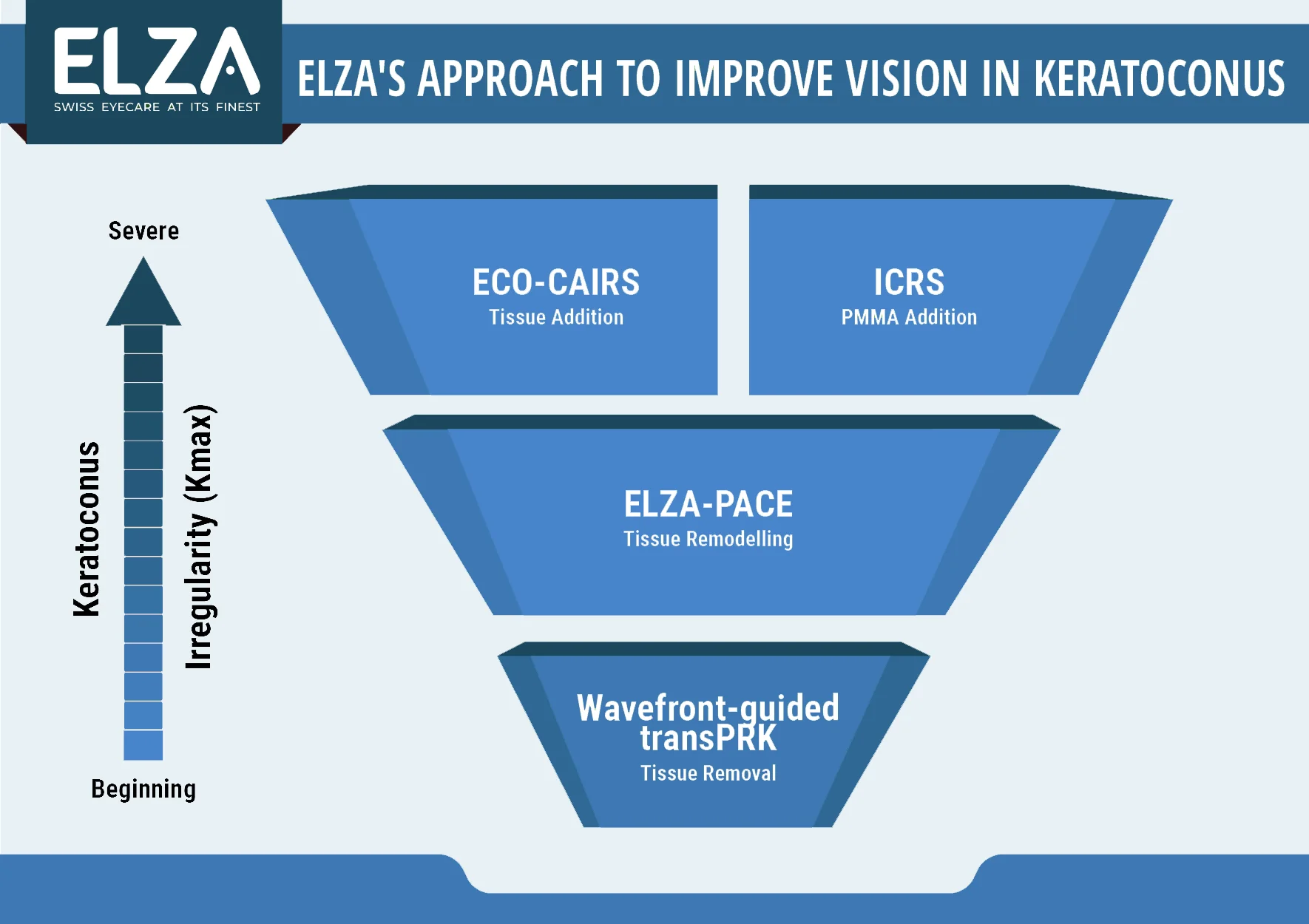
For patients with keratoconus, we can improve vision in both stable and progressing corneas by combining several treatment techniques. Special contact lenses, like scleral lenses, provide excellent vision enhancement, while surgical options aim to improve vision quality with glasses. Unlike cosmetic surgery, our goal isn’t to eliminate the need for glasses but to enhance the clarity and quality of vision through them. We offer four types of surgical treatments for vision improvement in keratoconus: corneal wavefront-guided transPRK, ELZA-PACE, All Femto-CAIRS, and Femto ICRS. Each method has unique benefits, and we’ll determine which approach is best suited for your specific needs. Often, we can use one technique initially and then apply a second procedure 6 to 12 months later to further enhance vision. It’s important to note that early treatment of keratoconus with CXL makes vision improvement easier with these methods.
PMMA addition
Tissue addition
No tissue removal
Tissue remodelling
Outcomes
Outcomes depend on how early keratoconus is diagnosed, whether it is progressing, and which treatment approach is appropriate. Many patients are able to maintain useful, functional vision with the right combination of monitoring, visual correction, and treatment.
For many patients, success means reading more comfortably, using screens more easily, and feeling more confident in daily life.
Good care includes clear explanations about what treatment can improve and what kind of follow-up may still be needed.
Keratoconus care is often about long-term stability and visual quality, not only a single intervention.
Learn more
FAQs
Keratoconus is an eye disease that affects the outermost layer of the eye, called the cornea. The mechanical strength of the tissue is reduced. This causes the cornea to bulge forward, forming a “cone” shape and resulting in irregular astigmatism The cornea may continue to bulge and thin out at the tip, increasing the amount of astigmatism over time. The fact that the cornea becomes so irregularly shaped means that spectacles can no longer be used to correct the visual effects of keratoconus effectively, although this is still possible with the use of special contact lenses in the early stages of the disease.
The main symptom of keratoconus is reduced visual acuity that cannot be fully corrected with glasses. In the early stages of the disease, the edges of objects can appear blurred and the disorder is particularly noticeable in the evening. As the disease progresses, double, triple, and even quadruple vision may result.
Literature has identified various factors for keratoconus development, such as genetic and environmental factors. Studies have identified several genes that may increase the chance of keratoconus. It is recommended to screen direct family members for keratoconus. In addition to genetics, excessive eye rubbing might be associated with the worsening of keratoconus.
Yes. Corneal cross-linking is a procedure that can stop the disease with a chance of success of over 90%. The idea of cross-linking was first conceived in Germany, but the technique and technology was developed in Zurich and has spread from Switzerland to the whole world. Today, CXL (corneal cross-linking) represents the global standard of keratoconus treatment.
Prof. Farhad Hafezi from the ELZA Institute was from the original group that established this technique in modern ophthalmology. He has one of the longest experiences in cross-linking in the world. Also, ELZA’s research group officially is the most productive in the history of CXL research.
Corneal cross-linking (CXL) is a technique that combines UV light (UV-A) and riboflavin (vitamin B2) to cause a photochemical reaction that mechanically stiffens the cornea by increasing the number of crosslinks in collagen and thus prevents further progression.
Corneal cross-linking (CXL) is able to stop the progression of keratoconus. Generally speaking, performing CXL makes sense when the disease is still progressing. The question of when to cross-link is closely linked to the age of the patient – but other factors factor into the decision making process, too.
This depends on the stage of your condition. Early-stage patients may need exams every 6-12 months, while those with more advanced cases may need more frequent visits. In children, we may need to examine the corneas every 4 weeks. Regular monitoring helps in detecting any progression so we can intervene as necessary.
Keratoconus very often begins with the hormonal changes in puberty. However, it is also quite possible that the disease is already evident in children. In 2012, the ELZA member Prof. Farhad Hafezi showed in a scientific study that keratoconus progresses in children and adolescents (8 to 19 years) with a frequency of almost 90% and worsens vision. It is therefore very important to carry out regular follow-up checks here.
No. Keratoconus is far more common than previously thought.
One of the most frequently cited scientific publications on keratoconus came from the United States of America in 1986 and stated that the prevalence of the disease is 1:2000, making keratoconus a rare disease. However, the equipment used at that time to detect diagnosis was far, far less sensitive than modern diagnostic instruments. What this means is that keratoconus is expected to be far more common than 1:2000 people – and if it’s thought to be rare, people might not be routinely screened for the disease, meaning that keratoconus might not always be detected early enough. Also, there are major differences in prevalence in different regions of our planet. In general, the earlier you treat keratoconus, the better the patients’ outcomes.
The study with the highest prevalence reported so far also comes from ELZA: in 2018, Emilio, Torres, Nikki Hafezi and Farhad Hafezi showed that the prevalence in children in Saudi Arabia is 1 in 21 or 4.7%.
With increasing age, our body (and the connective tissue it contains) becomes stiffer. Since the cornea is made from connective tissue (i.e. collagen), it becomes stiffer as well. Therefore, keratoconus will some day stop and not deteriorate further, often between the 35th and 45th year of life. However, we also see patients who still display active keratoconus inn their 50s: ageing only decreases the likelihood of keratoconus progression, but that probability will never be zero.
Yes, there are several ways to enhancing vision after in eyes with keratoconus.
All options are highly customised, and which option – or combination of options – are best depends on the individual eye. Notably, contact lenses, Femto-CAIRS, and wavefront-guided excimer laser treatments primarily serve to improve visual quality rather than address progressive corneal ectasias.
Corneal cross-linking (CXL) is unique in its ability to halt ectasia progression. ELZA’s pioneering ELZA-PACE customized cross-linking procedure not only strengthens the keratoconus to stop disease progression but also enhances visual quality simultaneously.
Yes, although the vision and image quality may vary depending on the severity of the keratoconus.
Unfortunately, on a global scale, keratoconus represents one of the major causes of legal blindness in the young, which is due to the fact that access to diagnosis and treatment is difficult in many countries. In industrialized countries, CXL has reduced the need for corneal transplantation by 50%, because keratoconus is detected and treated before it leads to major visual impairment. With corneal cross-linking and vision rehabilitation with the use of special contact lenses most patients can maintain good quality of life and functional vision.
Get in touch
During office hours.
Email us.
Make an appointment, and come to see us.
Thank you for writing a review on google.
Contact us here, we will get in touch with you.
Zoom online consultation for our international patients.
Contact us here, we will get in touch with you.
Contact us here, we will get in touch with you.
Stay informed & get the newsletter
You have successfully joined our subscriber list.
Newsletter abonnieren & informiert bleiben
Sie haben sich erfolgreich in unsere Abonnentenliste eingetragen.
Bitte bestätigen Sie Ihr Abonnement, indem Sie auf den Link in der E-Mail klicken, die wir Ihnen gerade geschickt haben.